Laparoscopic cholecystectomy
The surgery is performed under general anaesthesia and during it 4 small incisions (up to 2 cm) are made on your abdomen to allow the passage of the laparoscopic instruments. The abdomen is inflated with gas (carbon dioxide) so that enough room is created for the surgeon to perform the surgery with safety. The gas is harmless and gets absorbed very quickly by the body a few hours after the surgery. Once your gallbladder has been removed in the operating room, the gas insufflation of your abdomen will stop and the incisions will be closed with absorbable sutures. The procedure typically takes 1 hour and most patients get discharged from hospital on the following day.


Patients will be allowed to eat on the same day following their surgery and will be able to mobilise independently. Most patients return to their normal activities within 10-14 days from the day of surgery.
It is worth mentioning that between 1 out of 30 to 1 out of 40 cholecystectomies cannot be completed with the laparoscopic approach for a variety of reasons and in these situations the surgeon will choose to convert to an open operation in the interest of patient safety. Recovery following surgery will be slower in such cases.
What are the complications associated with laparoscopic cholecystectomy?
-
Bleeding (intra-abdominal/ incision sites) > rare
-
Bile duct injury > injury to the main duct (pipe) that drains the bile away from the liver may occur in approximately 1/400 surgeries.
-
Leakage of bile from the liver/bile duct to the abdomen > 1/100 surgeries
-
Injury to other organs such as the intestine or major blood vessels > 1/500 to 1/1000 surgeries
-
Retained bile duct stones
-
Hernia at the site of surgery (port site hernia)
-
Diarrhoea and excessive wind (flatulence) may be reported by up to 5/100 patients undergoing gallbladder surgery. The symptoms are usually mild and improve with time by making dietary modifications.
-
Thromboembolic events (blood clots lungs/legs) > low risk procedure
-
General anaesthetic risk > depends on the patient’s health status. All patients should undergo a pre-operative assessment by an anaesthetist.
Management of bile duct stones
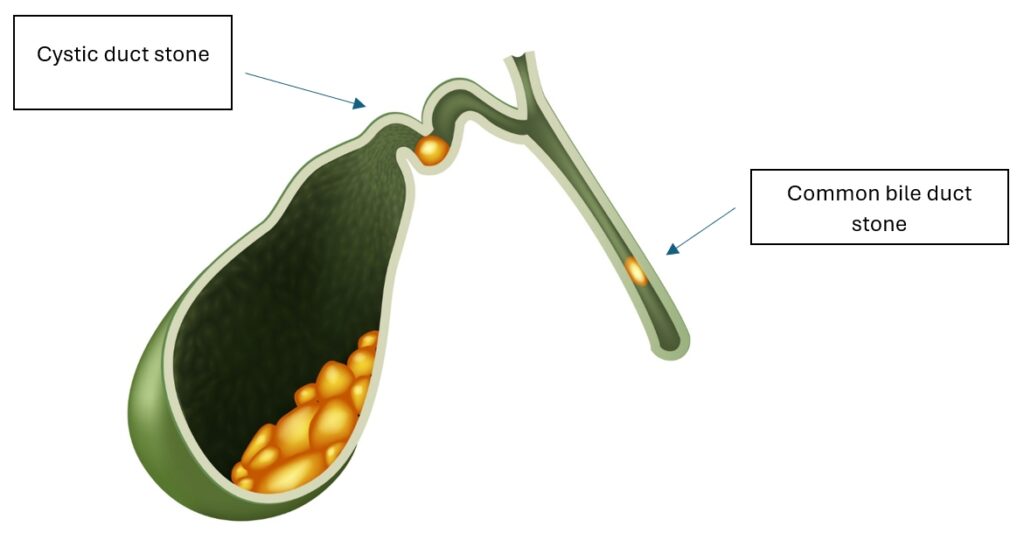
Stones in the Common Bile Duct (the main pipe that drains the bile away from the liver) usually migrate from the gallbladder itself. These stones usually present with one or more of the following symptoms: upper abdominal pain, jaundice (“yellow skin”), fevers or rigors.
Clinical suspicion of stones present in the bile duct can be raised when a patient’s liver enzymes (blood test) are deranged, even in the absence of symptoms. A MRI scan of your bile ducts and liver, and in some instances an abdominal ultrasound usually confirms the diagnosis.
Stones from the main duct may spontaneously pass on their own to the small bowel (the distal end of the bile duct) causing transient symptoms or blood test derangement. In cases where one or more stones block the lumen of the common duct, stone clearance is required in order to avoid secondary complications from their presence in the lumen either in the form of generalised sepsis or pancreatitis.
The stones from the duct can be extracted either with an endoscopic procedure called ERCP (a form of more sophisticated gastroscopy) or surgically by accessing the bile duct either by opening its front wall or through the small pipe that connects the gallbladder to the bile duct (the cystic duct). The procedure in experienced hands is usually done laparoscopically with a post-operative recovery similar to a laparoscopic cholecystectomy.
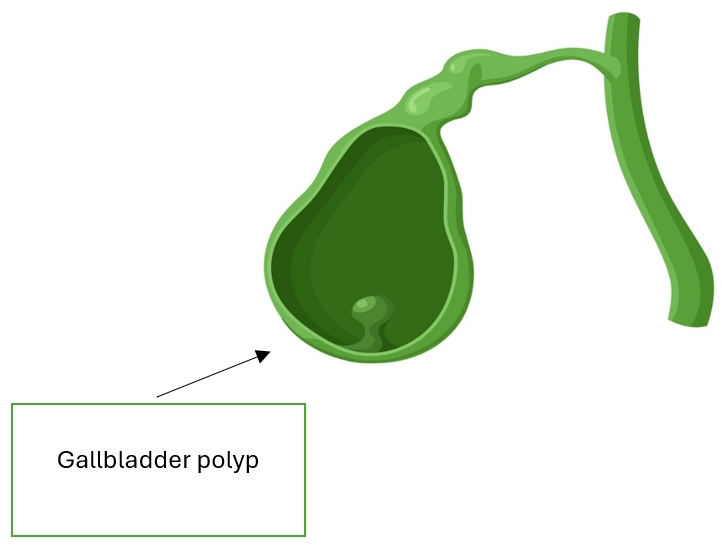
Surgery for gallbladder polyps
Gallbladder polyps are growths that protrude from the lining of the inside of the gallbladder. Gallbladder polyps typically do not cause any symptoms. They are often incidentally discovered on an abdominal scan when a patient is being investigated for other abdominal pathology. Studies have shown that larger polyps may harbour a malignant potential and therefore removal by means of cholecystectomy is recommended in some patients.
Below are the indications for cholecystectomy to remove gallbladder polyps:
-
Polyps larger than 1 cm in size (Ultrasound or MRI scan)
-
Single large polyp with wide base
-
Polyps presenting with gallstones
-
Polyps with rapid growths
-
Polyps that induce related symptoms (namely right upper quadrant pain)
-
Presence of polyps in patients with chronic liver conditions, mainly Primary Sclerosing Cholangitis
Should a polyp not meet the above criteria, monitoring by means of abdominal ultrasounds will be offered to the patient on regular intervals.
Sources for further reading:
The links below provide useful reading material for patients who need gallbladder surgery. They are provided by professional organisations.