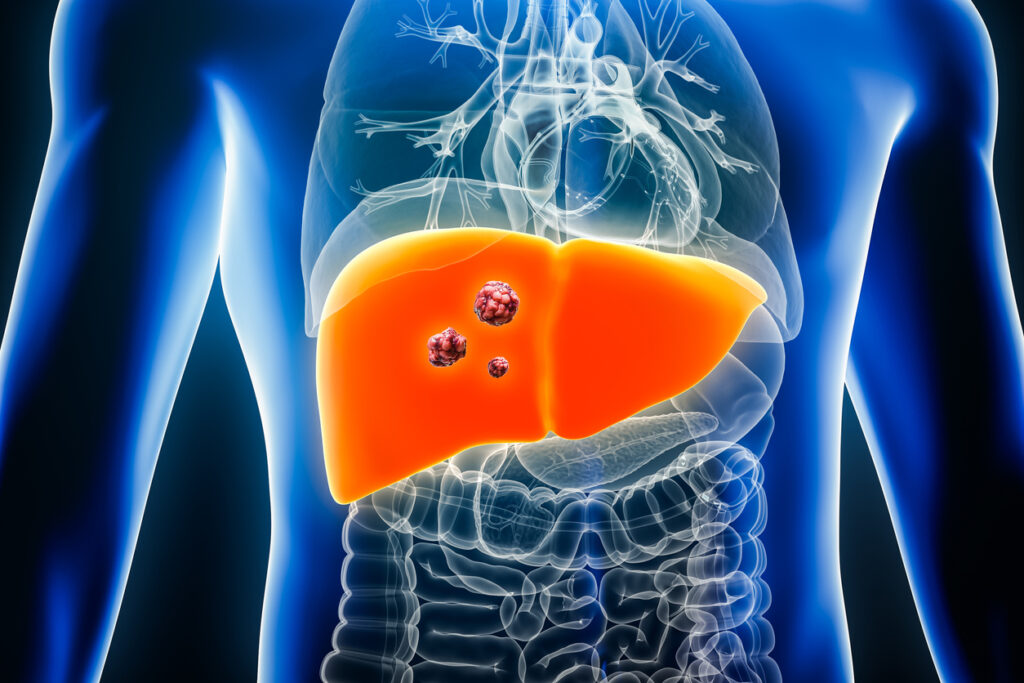
What are the types of liver tumours?


What is the treatment of liver tumours?
Liver surgery has entered the era of individualised patient care in terms of the management plan offered to each patient with a primary or metastatic liver tumour. In broad terms liver surgery as a stand alone therapy or in combination with other systemic or locoregional therapies (e.g. chemotherapy, immunotherapy, liver ablation) is offered with the aim of eradicating the cancer completely or removing metastatic disease, prolonging the patient’s survival.
All cases of liver tumours should be discussed in a structured Tumour Board meeting which is a meeting of cancer specialists including surgeons, radiologists and oncologists. The management plan offered to each patient depends on multiple factors including the type of liver cancer, the number/size of the liver tumours, therapies that the patient may already have had (e.g. chemotherapy) and also the medical background of the patient (e.g. presence of significant medical conditions such as ischaemic heart or chronic liver disease).
How complex is liver surgery?
The liver is a critical organ for all humans and has multiple critical functions including synthetic, metabolic and storage functions. Liver surgery is major abdominal surgery requiring advanced surgical skills by the clinician performing it. It can be performed either as a minimally invasive procedure (laparoscopically) or with the open approach depending on the location /number of tumours, the surgical history of the patient and the expertise of the surgeon.
The benefits and potential complications associated with this sort of surgery should be discussed in depth with the patient prior to deciding to proceed with it. A surgeon’s decision as to whether liver surgery can be offered to a patient may be influenced by the proximity of the liver tumour to critical vessels which lie next to the liver, presence of chronic liver disease (e.g. cirrhosis), the patient’s medical background and the amount of liver that will be left behind following the surgery as post-operative liver dysfunction is a major cause of morbidity. In many cases the patient’s surgeon and the oncologist may jointly decide prior to the surgery, to offer the patient a form of systemic therapy (e.g. chemotherapy) with the aim of shrinking the size or number of liver tumours in order to facilitate the surgery or reduce the magnitude of it.
What are the alternatives to liver surgery for inoperable liver tumours?
As mentioned above each patient should be offered a personalised management plan for their cancer treatment on the basis of their overall health and cancer status. Liver surgery is the treatment option with the higher chance for a cure for liver tumours, when selected appropriately. Technical factors such as the number of liver metastases, the location of the liver tumour in relation to critical structures such as blood vessels and the status of the background liver itself (e.g. presence of chronic liver disease) may preclude surgery, at least in first instance in some individuals.
Upcoming evidence in the literature suggests that other forms of systemic therapies (chemotherapy/immunotherapy) or local liver treatments such as ablation techniques (destruction of cancer cells with a “heat probe”) may be appropriate in selected patients as their outcomes have been very encouraging. Furthermore, there is evidence that these therapies are more advantageous for some individuals owing to the molecular profile of their tumours. These therapies can be used as an adjunct or a replacement to liver surgery depending on the patient’s physical status, type of liver cancer and size/location of the tumour. Furthermore, particularly in the case of systemic therapy (e.g. chemotherapy/immunotherapy) patients who were originally considered to be inoperable owing to the burden of liver cancer may become candidates for surgery depending upon their response to treatment.
It is therefore very important for all these factors to be taken into account during the consultation with the liver surgeon and the medical oncologist so that all options available can be presented and discussed with the patient.
Further reading:
The links below are provided by recognised professional bodies and provide reliable information for patient with liver tumours.